

Anterior Shoulder Pain??
As a physical therapist I have decided shoulder pain is the worst. Well, maybe after sciatica which seems to be much more painful. Anybody else have anterior shoulder pain? After having 3-4 months of shoulder pain, I am shocked at how difficult the shoulder can be to evaluate and treat—even on my own body. The pain started after a very long CrossFit workout with rowing, snatches, thrusters, and pull ups. As you can imagine it was a lot of shoulder work for around an hour. I am also shocked at how long pain can last even with conservative treatment. I think another reason pain in the shoulder seems to last longer, are the multiple areas of the shoulder that can get injured. For the longest time, I thought the pain was bicep tendinitis and very well could have been, but what I have found to be the biggest contributor to my pain, once other area of inflammation subsided, is pectoral tendinitis.
The pain was mostly in the anterior shoulder and hurt mostly with raising the shoulder, also known as flexion. I remember reaching over to turn off a lamp and having a lot of difficulty. There was also pain anytime I reached behind me or extended my shoulder. Especially, when resistance was added like closing a door. The AC joint was painful and for a period of time the whole shoulder felt like it was inflamed. With the help of a friend who had ultrasounds diagnostic I could confirm there was bursitis and AC joint inflammation. This is why the whole shoulder felt painful at times and why the pain felt everywhere. Over the course of months, as the shoulder felt better, specific movements became painful such as resisted flexion and especially horizontal adduction+
As with most things, it’s not hard to figure out what is wrong but how it got inflamed and how to prevent it from happening again can be more difficult. I would like to review the primary diagnosis first and on later post review how it got injured. Also lets look at how to rehab it and how to prevent it from happening again.
The pectoral muscle has two functions besides bringing your arms together like a dumbbell fly. The pectorals also flex and extend the arm. There are two different sections of the pectorals that accomplish this. The sternal head helps extend the shoulder and the clavicular head helps flex the shoulder.
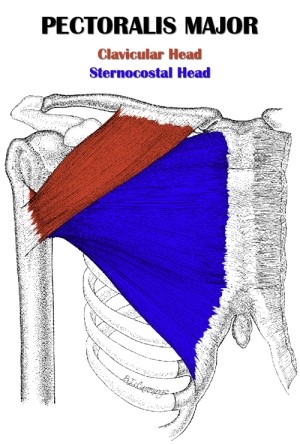
Since my pain was mostly with flexion and horizontal Adduction, it was easy to tell that the clavicular head was more at fault. Looking at where the clavicular head attaches makes it easy to see why it is hard to diagnose with so many things attaching to the anterior side of the upper Humerus. The deltoid/biceps/subscapularis/bursae/labrum are all possibilities that could create anterior shoulder pain. Also it is easy to see why the AC joint was irritated with the clavicular head attaching on the clavicle. ON the next post I would like to discuss helpful positions that help diagnosis it.










